Presented by Emma Riebi, LPC, LMHC, and Christine Stokert, RN
Collaboration between the disciplines of eating disorder treatment can have a significant effect on patient outcomes. Nurses and therapists are often seen as operating in opposite treatment disciplines, but at their presentation at the 2023 Within Health Summit, Therapist Emma Riebi and Nurse Christine Stokert discuss the ways their fields can collaborate to benefit eating disorder treatment.
A multidisciplinary approach is the gold standard of care for eating disorder treatment; as we know, eating disorders are biopsychosocial disorders, i.e., they affect a person physically, mentally, socially, psychologically, and spiritually.
For eating disorder treatment, a multidisciplinary team consists of medical, psychiatric, psychological, and nutritional expertise:1
Qualitative studies have shown the importance of high levels of collaboration between multidisciplinary members. It is:2
Many people still hold onto the perception of the stereotypical therapist who sits on a couch and talks to people about their feelings, which ultimately “fixes” them. This very idealistic view doesn’t accurately represent how therapists are trained and work.
Therapists are trained to take a client-led approach, i.e., instead of “fixing” the client, a therapist helps the client come to their own solutions, as well as tap into their own sources of healing and the support systems in their lives. In eating disorder treatment, therapists do the following:
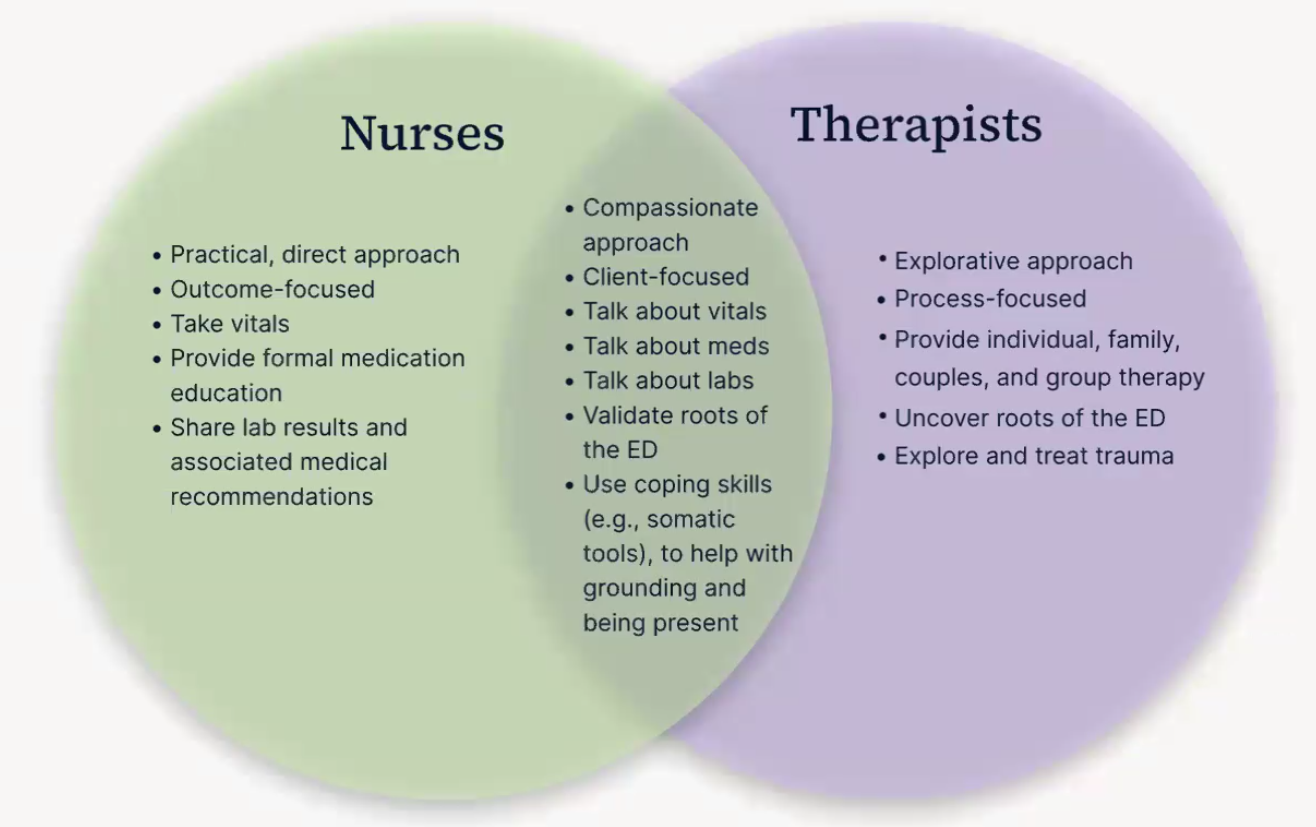
There are several elements of eating disorder care where there is a significant overlap between nurses and therapists, as the above Venn diagram shows. Nurses and therapists can step outside their “lanes” to come together to help clients move forward in their treatment.
Inpatient and outpatient eating disorder clients are often medically fragile. When medically-compromised clients enter eating disorder treatment, collaboration between disciplines is important.
When a client has a high level of medical complexities, these concerns can often “hijack” therapy sessions. This is where nurses can become key allies to clients, addressing medical concerns and allowing a therapist to focus on the root cause(s) of eating disorders, such as trauma.
Additionally, nurses and therapists can come together in a session to converse with clients from both therapeutic perspectives. Furthermore, collaboration between therapists and nurses provides an excellent opportunity to learn from one another. Being informed about the goings-on with a client in other disciplines enables all-around support of a client's treatment for the best possible outcomes.
Collaboration between therapists and nurses requires:
It’s well known that many eating disorder clients have one or more co-occurring psychiatric disorders. There is usually a typically complex interplay between these co-morbidities, which requires treatment of the person as a whole, i.e., treat all co-occurring disorders at once. This is where it becomes key for nurses and therapists to work together, particularly when it comes to medications.
Neither nurses nor therapists prescribe medications and, therefore, can provide more objective information on recommended medications and address any concerns a client may have from different, yet complementary, standpoints. For example, a nurse can inform a client about the biomechanics of how a certain medication may work, potential side effects, and how to take it. At the same time, a therapist can discuss a client’s beliefs about and barriers to taking medication.
Collaboration between nurses and therapists can improve:
The “opposite” approaches of therapy and nurses can tackle different client barriers. For example, nurses can offer fantastic support in helping clients attain and refill their prescriptions, as well as put a routine in place for taking their medications at the right time.
Often, nurses are not considered part of family settings. However, nurses can and should be utilized to provide complementary skills and approaches to therapists.
The case of Client A provides an excellent example of how collaboration between nurses and therapists looks in reality and leads to positive patient outcomes.
About Client A:
The treatment plan for Client A focused on decreasing eating disorder behaviors while not engaging in self-harm behaviors or engaging in disordered earring behaviors to soothe anxiety. Treatment also included following up on Client A’s medical appointments.
The treatment modalities used included dialectical behavioral therapy (DBT), acceptance and commitment therapy (ACT), internal family systems therapy (IFS), and solution-focused therapy. Nurses and other members of the multidisciplinary team also worked with Client A in utilizing the skills learned in DBT and other therapies, contributing to positive treatment outcomes:
At the time of admission, Client A had had clinically significant elevated scores across the board. By the time of discharge, Client A was at or below the clinical threshold, experiencing a reduction in eating disorder symptoms, an improvement in quality of life, and a significant reduction in depression and anxiety.

The outcomes of Client A are a testament to how well therapy and nursing work together. A prime example of nurse and therapist collaboration was with the client’s trouble with their sleep apnea machine.
Face coverings were very triggering for Client A. The therapist worked on addressing the client's trauma while the nurse worked on getting them to understand how important the sleep apnea mask was for their health, as well as reinforcing the work of the therapist. This resulted in Client A using their sleep apnea mask for the first time in years.
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur.
Block quote
Ordered list
Unordered list
Bold text
Emphasis
Superscript
Subscript
